This post depicts the act of turning an animal into food.
Some may find it gruesome, which may be indicative of a disconnect that is ultimately unhealthy for you and possibly more dangerous to the animal’s welfare.
Many of you know it as Head Cheese or Brawn, if you’re British. Some confuse it with Scrapple (Head cheese + corn meal) which is similar to Goetta (with oats) which is popular in Cincinnati. It can be made into a Terrine, or loaf and sliced for sandwiches, but I prefer to prepare it the way my grandmother did, which is canned in mason jars. As a kid we used it as a sandwich spread, but I spoon it out and pan fry it.
My particular Hillbilly heritage hails from the Big Savage Mountain area of the Alleghenies. We’re from Frostburg & Cumberland, MD and Salisbury, PA. We’re mountain folk who tended to be Methodists, whose preachers had no church hall, but rode a circuit on horseback with little more than a blanket- traveling to the isolated hillfolk to spread the Gospel. We are also the type of hillfolk that call headcheese,”Souse”, which is also how we describe being drunk. Getting “soused” and staying “soused” is all my people had to do when snowed in from harvest-time to spring thaw.
Heh, “My people”.
I am fortunate enough to be able to source pig heads from a local farm called New Creation Farm. I understand that in some parts of the country, Walmart carries frozen pig heads. God Bless. But I try to source local meats from places where I am fairly certain I am aware of their husbandry practices.
“Mommy, Can I eat it now?”
This is how you sneak a pig head into the house. This is all your wife should see until the canning is done. Even then, it’s best to have a hiding spot in the basement (not for the processed jars, for you). Take a spoon.
Prepare your work-space out of doors, if you can. Especially if your wife has locked you out of the house.
Here’s how it looks when you first unwrap it. It needs a little shave. Some people have a (hopefully) dedicated straight razor just for this job.
I, however, just use a torch. Don’t forget to get deep into the ears.
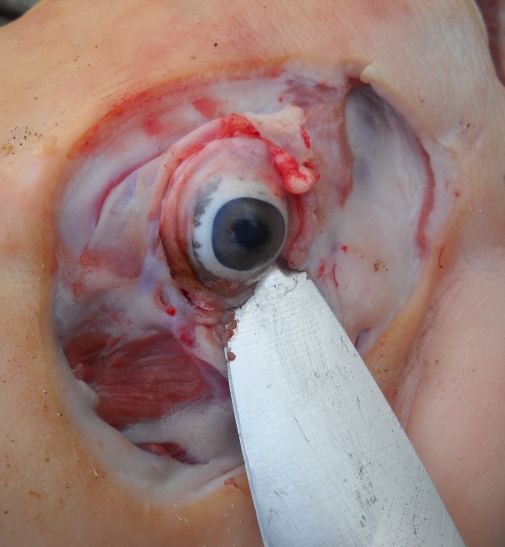
The Foxfire Book‘s second chapter concerns a couple of young guys who are helping an elderly lady named “Aunt Arie” butcher a pig head. There is a humorous moment when she digs one of the eyes out with a butcher knife and flings it outside, onto a near-by tin roof and it rolls off and hangs “bobbing on a clothes line”. They ask her if it bothers her and she replies, “I don’t care fer’t bit more’n spit’n’th’fire”.
That is not a great way to accomplish this job. I now pull on the eye with a pair of needle-nose pliers and cut the optic nerve with a pair of kitchen shears.
There is a Department of Agriculture stamp. I don’t know if it’s edible. I cut it off just to be safe.
I also remove the ears. Some people don’t, they add it to the Souse. But some complain that the ears are too gristley. I don’t know because I don’t want to risk making a whole batch that is not to my liking, so I remove them just in case. There are recipes out there for just the ears, so maybe I will try one of those one day but it hardly seems worth it for two ears. I throw these into the woods for the animals and let the thought of one of the neighbor dogs running home with these or a skull entertain me.
Next I cut them down to stock pot size with a Sawzall fitted with a long wood blade. You see here in the cross section the hog jowels- pretty much the most delectable meat on the planet. Like a butt roast, it is strong, well-used muscle that must be cooked slow and low into a mouth-watering thing of beauty.
If you can get a hold of some trotters, they add a lot of gelatin (aspic) to the mixture and help a lot when trying to get this to set up if you choose to make a loaf instead of canning it.
You can throw anything you like in at this point. Use spices, trotters, herbs (traditionally Sage), vegetables-whatever suits your fancy. This is your time to make a personal recipe they will be begging for at the company pot lucks. If you are uninspired or not handy with spices, search for bone broth / soup stock recipes and use those spice mixtures. Here’s a simple one that I enjoy. Start here and let your imagination run wild.
Next boil it forever. The longer you boil it, the more you will cook out of the bones. I suggest 6-8 hours at minimum. I often simmer it overnight and if I can stand it, 18 hours. This would be a good project on a wood stove.
I was visiting my cajun-country friend not long ago and he had recently taken his kids on a pig hunt. Feral animals of the Porcine persuasion are BIG TROUBLE in the South and they are heading north. They are super-aggressive, a threat to children, property (I’ve seen full-sized pig roadkill – imagine THAT crash!) and the environment. If you go on a feral pig hunt, you are a hero to society. Them Cajuns trap wild piglets and raise them in pens for a season or two. WHAT A LIFE, Guys!
This is “Rooty”.
So my cajun-country friend and I decide to make some souse in a a Crawfish boiler. Taking a cue from the bone broth recipes, I had been adding vinegar early on in the water to leach calcium out of the bones. I said, “OK, add a bunch of vinegar”. I meant a few good splashes. After I heard about the 10th, “glub-glub-glub” I looked over to see that he had added about 1/3 of a gallon of apple cider vinegar.
“Whoa! Dude! That’s a lot!”
Here I am coveting. I need one of these crawfish pots SO BAD!!
I was worried, and for a moment assumed we had ruined it. But the end result was delicious. He set it up as a loaf-style terrine. And the skull was so soft I could crush it with my hands (but I left it for his kids to play with). That bony goodness was now bio-available, set in aspic. For the love of Ted Nugent. So don’t be afraid of vinegar.
Next, remove the head from the water. Be careful because it is pig-fat slippery and will fall apart and splash into the boiling water if you’re not careful. It is easy to pick the bones out at this point.
A quick hammer whack will get you to the brain. Be sure to keep yelling “BRAAAAAINNNNNN…MORE BRAINN!!” to the annoyance of those around you.
(no one will be around you)
I try to grind it as fast as possible so that I can hot-pack into the Mason jars. Or I keep it hot in an electric skillet, either loose or in unsealed jars. Try not to think about The Wall. Damn You, Roger Waters! Or if you’ve ever been to a GWAR show…
The stock that is left behind will settle into 3 layers: a snow-white mild lard that can be used for baking, a dark, flavorful lard that is similar to bacon grease, and a thick, rich bone broth that can be used for soup stocks, making rice or drinking, etc…
If you cook a long time or add a trotter or two, the bone broth will be so thick and gelatinous, you can stand a heavy spoon in it once it chills. Lovely for your hair and nails. Also it is a source for much-needed Glycine.
If you are on a budget, this is the way to feed your family. A $15 head will give you several quarts of stock and many pounds of meat. One day I will figure out the calorie price. You can’t beat this anywhere and it’s such nourishing meat.
I’ve been experimenting with smoking the head instead of boiling. I was VERY happy with this. And the big pressure canner is big enough to accommodate a whole head. I don’t need to use the sawzall.
Since I don’t have a great smoker, I finish it in a pressure cooker with very little water – you can still the Stock spices if you like. When you do it this way, you don’t lose the fats into the broth. It gets mixed in with the meat canning. The smoked head is hard as shoe leather. Once again, I was convinced I had ruined it, but it softened beautifully in the pressure cooker.
This is what a smoked head looks like after pressure cooking. Spooky, no?
Here’s a jar of smoked souse in front of “regular”. It has a very rich, dark color and visibly more fat- great for us ketosis junkies.
Here we’re packed and ready for the canner. Use your canner’s instructions.
I’ve even tried a dry brine. I like what “Meathead Goldwyn” has to say about dry brining as opposed to bath brining over at Amazing Ribs. I also find this science of brining article helpful not only for meats but Lactofermentation of vegetables.
My favorite preparation is just nested within (or next to) a bed of Collard or Mustard greens. Here, served with the bone broth and pink salt. I also love to toss the greens in flavored vinegar.
Another is rolled into steamed or blanched Chard leaves which are crisp and bitter enough to mitigate the high-fat mouthfeel of the souse which is salted and cooked to just a little crisp. I just need to come up with a sauce now. I’m thinking Sage-based. I may add a filler (more greens?)
And at the end of the day you have a new toy! Play ‘Lord of the Flies’ or make a scarecrow or marionette. Give it to the kids for crafts. Or just hope one of the neighbor dogs picks it up. It’s the gift that keeps on giving. I usually chase my wife around with it, making it yell, “Sucks to your ass-mar, Piggy!”
I will keep updating this post as the experiments continue.
Lastly, the number of youtube videos about this this are finally growing but here is my favorite. Dude just cuts it off the skull and rolls it into a loaf. Forgive his hairstyle. I will definitely be trying this technique one day. I think I need a better knife first.
My health coaching certification is through Mark Sisson’s Primal Health Coaching Institute. I chose it because I agree with just about every conclusion Mark has come to based on my own research that started about a decade before I found Mark. But even Mark has said, “Maybe the term ‘Primal’ doesn’t have to stick around.” Why? It’s just an ideal.
First,
What is this “Paleo Diet” or “Paleo lifestyle”?
Agriculture was the “Worst Mistake in the History of the Human Race”
~Jared Diamond
Though any simpleton could characterize it as running around with a bone through your nose, killing animals with stones and eating their flesh raw. It is actually merely a quest to figure out just what this human animal’s diet really should be. It is fairly obvious that we have lost track of this as technology-starting with agriculture- has advanced. So when I see someone claiming to “debunk” the Paleo diet, I have to ask ‘WHAT Paleo diet”? The concept doesn’t really belong to anyone, though many claim it. Loren Cordain’s Paleo diet? Robb Wolf’s? Nora Gedgaudas’? There is no official ‘Paleo Diet’. Are they debunking the concept of the Paleo diet? As if humans ate incorrectly for millions of years and didn’t get it right until we had steel-cut oats?
And the quest for our true, healthiest diet isn’t even that. It’s actually a quest to ascertain which neolithic innovations and habits are the causes of unnecessary morbidity and early mortality, which is suddenly important to us now that life expectancy is decreasing for the first time, ever, in the richest countries in the world. No one in this Paleo “movement” is against technology per se. This brings us to Mark Sisson’s ‘Primal’ construct.
What is this “Primal Diet” or “Primal lifestyle”?
Mark Sisson is not a scientist like Loren Cordain or Chris Masterjohn. His not a Physician like Doug McGuff. He’s a guy with a good mind for science who takes the time to review the mountains of data produced by scientists and physicians and organize it into a cohesive lifestyle plan with the twin goals of not taking years from your life or life from your years with these so-called neolithic agents of disease. “The Primal Blueprint” is his branded version of the Paleo vision of optimal health. “Blueprint” refers to the influence of your DNA on your health and refers to your ability to “tune” your DNA expression through epigenetics.
But he recognizes that there are neolithic agents, discoveries and technologies that are truly beneficial, such as computers (when not abused), electronic heart monitors, Lactobacillic fermentation, dark chocolate, Dairy-if you tolerate it, or non-insulinogenic natural sweeteners that require modern processing or even distilled spirits! Mark calls this “Primal Living in the Modern World” and his critics like to point out these individual nuances as hypocritical or “not so primal” with snarky glee. But they are missing the point and really just show that they aren’t reading his work. This situation can be confusing for neophytes, too. “How am I ‘Primal’ and preparing food with airlocks and drinking Tequila, again?” Well…
Some of Mark’s inconsistencies are a little hard to carry water for, though. He has claimed to dislike “Primal Analogues of Neolithic agents of sickness” (i.e. primal chocolate muffins) but shares recipes for just such things all the time. I guess science must always be revised and his concept of “Primal Living in the Modern World” is getting looser. That does not, however, dismiss his basic concept that you can be in control of your body and play your metabolism like a fiddle once you know what’s going on. Once you accomplish this, you’ll know how to let these cheats in.
That’s why I say let’s skip the whole ‘vocabulary’ business and refer to this work when needed. Words are incredibly limiting ways to express abstract concepts, anyway. I happily draw from the experience of Vegans, Ayurvedics, Paleos and Primals, holding the feet of each to the fire of scientific scrutiny based on my own understanding of modern science.
I am not going to coerce anyone to “go Primal’, but if you want to, I’m the guy to tell you how and why. And of course I will advertise to draw those people, too.
You may see a pro-vegan/anti-paleo blog post that reads, “No, pasta is not killing you”. This is true. Chronic hyperinsulinemia is what’s killing you . Pasta is just one quick way to get to hyperinsulinemia. So are sugary beverages. So is coffee cake. You choose the form of The Destructor, Ray. I can show you how to navigate those waters with reason, logic and good, old-fashioned book science. And the paleo scientists are pretty sure there wasn’t tons of hyperinsulinemia around 15,000 years ago.
Lastly, thanks to hearsay, social media misguidance and irresponsible journalism, some may come to the Paleo/Primal philosophies with a jaundiced view (that’s a liver joke! Get it? Hepatocellular build up of excess bilirubin!). They may think it’s trendy or a fad and stop listening to good information based on that. Of course this kind of intellectual bigotry is not really my responsibility, but I circumnavigate it when I can. The Paleo guys claim quite the opposite; in the Geologic scale of things, even farming is new and trendy at 12-15,000 years young and processed foods are a lightening flash that hasn’t faded away from vision just yet. They want a new understanding of what “optimal” is that isn’t shaped by lobbyists, superstition or activism science.
According to emergency room Doctor Doug McGuff, the American health care system is collapsing and some say by design. That may sound conspiratorial, but anyone can see that we’re increasingly getting less for a higher cost in an environment of skyrocketing technological advances. This is the wrong time for almost 90% of us to be metabolically unhealthy, mostly by our own actions, informed or innocent.
Aside from being a proponent of the ‘Super-slow’ High Intensity Training (H.I.T.) exercise movement, Doug is a major force in explaining to people why it is imperative that we become healthy right now and not a day too late. To paraphrase him: Your #1 job for the rest of your life is to stay out of the Belly of this Beast (meaning our healthcare system). Personally, I find him to be a Philosopher-King and have yet to find disagreement with any of his words. He elucidates this in his book, “The Primal Prescription: Surviving The “Sick Care” Sinkhole“.
Previous to this book, in a 2012 Talk entitled Fitness, Health, and Liberty, Doug explains what exactly is already irrevocably around your neck and only going to tighten over time by giving a history of our healthcare system over the past 100 years. There is something in it for the liberals because he’s going to beat up on the Big Business. There is something in it for the conservatives because he is going to indict The Government. He will undeniably show how everyone involved, including doctors and 100 years-worth of voters are at fault for this mess. We know who the enemy is, Pogo.
I have painstakingly transcribed this talk for you for review of and comment upon. If you pinch the text, please give me transcription credit. But this labor is my gift to the world.
If you have neither time to read this nor watch it, I suggest making an MP3 out of it and listening during a commute, mowing the lawn, running on a tread mill, etc. I have never met someone who stands to learn nothing from this lecture. Doug will:
Demonstrate well-meaning, community-intended ideas that came with criminal fiscal irresponsibility.
Explain why your inner city emergency rooms look like 19th Century Flop Houses.
Show why everything medical you do is at an out-patient center
Parse out details such as: HIPAA is not for your confidentiality or assurance of consistent records-it hides the collectivism trumping your personal rights.
List the consequences of major political acts from Blue Cross and The Hill-Burton Act to EMTALA to Obamacare.
~Jimm
~~Begin Transcript~~
Normally I talk about exercise and diet but there’s not anything that I can tell you about exercise that you are going to remember that Skyler did not cover beautifully yesterday in his lecture so if you’re watching this on video, go watch Skyler’s Talk and you will have everything you need to know about exercise in that talk. Likewise, with regard to diet, there is nothing that I could tell you today that you are going to remember that wasn’t beautifully covered by Jolly or Dave Asprey in their talks today. So I would reference those for you. So instead of like in 2010 me telling you the how of the Paleo diet and the how of exercise I wanna tell you why. And I wanna do that from a very unique perspective and that perspective is: 23 years practicing in the epicenter of the implosion of the American healthcare system.
If you care about your liberty and preserving it, you need to care about your health. Now, everyone that’s sitting on an aisle seat on this side of the room, please raise your hand. OK, everyone look around for those of you that are younger than 35-years-old in this room, statistically speaking, this is the number of you that will be dead before you are 35. Keep your hands up. Everyone on this side of the room please raise your hand. That is the number of people, statistically speaking that is going to have a serious life-threatening health condition or injury before they reach age 35. That’s why this is important that is why I want to talk to you about fitness, health and liberty: preserving personal freedom by staying out of the Belly of the Beast.
Now one thing that I want to make reference to as we go through all this is remember that every step of the way in this story that I am going to tell you. When we made a mistake or did something wrong, we never go back on that mistake. This is true of individuals but it is particularly true of bureaucracies and government. If they make a mistake that did not work out, well they never go back on it. They always double down and do even more of it.
So, medical care. What is it? What should it be vs. what it is. What medical care should be, is a free market exchange; a fiduciary relationship between the provider of a service and a consumer. The moment that you engage me as a physician, I should have a fiduciary relationship to you to take your best interest at heart. But what is it actually today? What it is, is a 3rd party relationship where the provider is coerced to place the needs of a collective over the needs of an individual. Now in a proper circumstance when you engage me as a physician we would be discussing both the price and the extent of the care that would provided up front.
As it stands nowadays if a patient’s coming through the E.R. even with something as simple as a laceration and they ask me, “Doc, what’s this going to cost me?” I have no idea what to tell the patient. If you get admitted to a hospital you have no real means of negotiating what your extent of treatment is going to be. In most cases, the extent of what is provided to you would be way beyond what you would normally negotiate under a correct provider / recipient relationship. The other thing that happens is: instead of you getting to decide what you want and what you don’t want, whether you want a statin or not want a statin, you kind of get a take-it-or-leave-it attitude because the system is now protocol-driven. If you don’t fit in to the protocol or accept the protocol…you know, there is no negotiation. It’s all or nothing.
So who’s to blame for all this mess? [points to self] Doctors.
This is an important point for all of you. Whenever anything is screwed up in your life I want you to say four words: It is all my fault. Five words? It’s all my fault. Assume responsibility for everything that’s screwed up in your life. Doctors did this to ourselves. The doctors that did it did it with short-term gain in mind, and they probably knew that the consequences of this would not be born in their lifetime but in the life time of future physicians and future patients. But they sought the help of the Government for short term gain and they set in motion the long term unintended consequences that has resulted in our ultimate enslavement. So what’d they do?
Anyone ever heard of Blue Cross and Blue Shield? This came about in the Great Depression. Now before the onslaught of everything that we currently have, a lot of physicians provided a very large mass of charity care and during the Great Depression- a calamitous economic event triggered by Government regulation – not many patients were being paid for their services. This is where you heard about doctors being paid in chickens and eggs and milk and what not because this is all that people had to exchange with. The medium of exchange had gone down to that. That they devised was an insurance system whereby they were guaranteed to receive a payment for their services but they bastardized what insurance actually is. What insurance should be is you pay a premium along with a lot of other people that goes into a kitty that will pay you should you encounter some catastrophic unforeseen event, but the insurance structure that they made was something to pay for everything: routine office visits, medications, screening tests, the whole nine yards. Come to the office with an ear ache or a sore throat, it was under the umbrella of this insurance that you paid premiums for.
Furthermore, they sought a tax-exempt status. What they wanted to happen was people that were buying their insurance plan was for them to be buying that with pre-tax dollars. Normally when you buy insurance, when you buy automobile insurance…when you buy life insurance, you buy it with post-tax dollars. That means if you made $100 the government takes $40 and leaves you with $60 and you buy your premiums with that. When something is allowed on a pre-tax basis, you get to buy it with the $100 you originally made. So in essence, you’re buying it at a 40% discount. Well the Government said “OK, we’ll do that but what we want in exchange for that is a community rating.” Does anyone know what a community rating is? Basically what that says is: anyone within a geographic catchment area pays the same premium regardless of their pre-existing health status. So that’s created layers of what are called moral hazards.
So what’s Moral Hazard? Well, Moral Hazard just has to do with what your behavior is under different circumstances. Let’s string a tight rope on the top floor of this building across the street to the other building. Well, Moral Hazard is the difference in the way you behave on that tight rope when there’s a safety net eight feet below you versus when there isn’t. So people’s behavior was changed by the fact that they were covered for everything. The consequences of not washing your hands or eating something that sat out for too long were now much smaller. You didn’t have to pay if you got sick even for the most minor of illnesses. More importantly, you felt as if you were going to be taken care of even if even got a more major illness that occurred as a result of your behavior over time.
So this was great for the doctors at the beginning of the medical Ponzi scheme. But not so great for those of us down the line. So- what happens next? Well remember this is occurring in a medical market where different providers are competing within that market. So, commercial insurers tried to compete. People that aren’t Blue Cross / Blue Shield that don’t have the pre-tax benefit- they have a lack of tax-exempt status, they’re forced to compete by offering a similar product. So what happens then is the concept of third-party payment for medical services becomes entrenched. This essentially becomes pre-paid medical care. This makes comparison shopping near-impossible because you’re not comparing price as you would in an open free market – its premiums and it creates another moral hazard that’s called Friedman’s Quadrants. And it refers to Milton Friedman.
And I wanted to have a white board up here to draw it for you but to spare us all the rigmarole of trying to get that thing up here let’s just divide this screen into quadrants. And on one side what we’re going to have is your money and then below is going to be someone else’s money. That’s the Y axis. So on the Y axis, we’re going to have your money and someone else’s money. On the X axis, we’re going to have yourself and someone else. So, when a person spends their money on themselves they’re going to worry very much about the price and they’re going to worry about the quality of what’s supplied. That is where the most conservative economic calculations occurs. Now if you’re going to spend your money one someone else, you’re still very concerned about price but you’re not quite so concerned about quality. You’re buying a birthday present for someone and you’re like, “Eh, I think they’ll like it. Maybe they’ll hate it. I will never know so I don’t really care that much.”
So down in this quadrant you’re going to spend someone else’s money on yourself. And that’s kind of where we’re starting off with this. There, you don’t care so much about price but you care about quality and you want to make darned sure that you get the quality you want but you don’t really care what it costs someone else to provide you with what you want. This is sort of the equivalent of being a welfare Medicaid recipient. And in the last quadrant is the worst kind of spending you can do and that is to spend someone else’s money on someone else. When you’re in that quadrant and you are spending you don’t care about the price and you don’t care about the quality. And when you create a third party payer medical system, that’s what you have.
Your money
Spent on Yourself
Your money
Spent on Someone Else
Someone Else’s money
Spent on Yourself
Someone Else’s money
Spent on Someone Else
People are not buying their healthcare in a direct transaction. Healthcare is bought with premiums that you have no idea what the cost is and you don’t care. How many of you people are employed and covered under employer insurance? Do you know how much it costs you every month? We got one guy? Do you know how much comes out of your paycheck? Dollars and cents?
Audience member: “$92…126?”
It’s variable but the number of employees that actually know what’s being taken out of their paycheck and whether those are pre or post tax dollars and all sorts of … If you go to an ER do you know how much you’re going to pay?
Audience member: “Just my deductible, 100 bucks”
So you pay a hundred dollars and you’re covered 100%? You don’t have an 80/20 or anything like that? So most people – they don’t know how much is being taken out and they don’t know what’s it’s going to cost when they show up for care. So this creates another moral hazard because you’re down in this quadrant- you don’t care about price, you don’t care about quality.
So, the situation was made worse by the 1942 Stabilization act– we’re in the middle of WWII. A lot of America’s men in the work force are off fighting war. And the thing you’ve got to realize about labor is like anything that’s bought and sold, or anything that’s scarce it has a price. So wages could potentially go up during this time of economic hardship which could put a real strain on employers so there’s a lot of political pressure to freeze wages and that’s what they did. But all of a sudden, employers were hamstrung for competing for very limited labor supply. So what happened then is the government allowed employers to compete for scarce labor by offering benefits such as their health insurance to not be considered in the wages act. What happens then…is these are pre-tax dollars and they’re not taxed and that amplifies this whole effect. So remember price controls will always create shortages. They applied price controls on wages which created a shortage a shortage of labor. So they had to find an end-around and their end-around was to offer benefits or things that were not counted as wages under the act.
Then what happens? The IRS gets involved. In 1943, they made certain that any premiums paid by employees in a group plan were exempt from federal income tax and they decreed that health insurance premiums are now legitimate cost of doing business and they can be deducted from the employer’s taxable income, too. So this has collectivized things both on the employee and the employer side. So collectivism is incentivized. So these tax incentives were available to anyone that got their healthcare collectively through employers but it was not applied to individuals who individually bought their insurance policies for themselves who wanted to stay independent, who wanted to preserve as much as possible that relationship between themselves and their doctors so they were financially punished for trying to remain independent.
So what are the logical consequences? Employees become unaware of the cost of what they’re seeking. And because it’s bought with pre-tax dollars dollars and there is no apples to apples comparison of what that really means in terms of your salary. Especially since taxation rates are gradated. The first money that you make is taxed at a lower rate than the middle money that you make which is taxed at a different rate that the top-end money that you make. So it makes it very hard to form any economic calculations. Employers insure the group without any concern for the given individual’s circumstance so you may have very peculiar or particular healthcare needs based on pre-existing conditions, congenital problems…but it doesn’t matter. They’re insuring the collective- the whole. That’s their concern. There is no concern for the individual anymore and worst of all it feels like an entitlement. It feels like something that just comes along with being employed. When I’m employed, I have “benefits”. I’m covered for my health insurance. And it engenders a buffet mentality. You’ve paid in a certain amount for your premium and now when you go to a buffet there’s a lot of food in front of you and you have to pay $14 to go the buffet are you really going to stick to your diet or are you going to get your money’s worth by gorging yourself? That’s the problem with a buffet. And that’s the problem with the logical consequences of making this sort of system.
So then what happens next? Well, prior to 1965, there’s always been indigent care. There’s always been a need to care the poor or the elderly who became destitute, either because of their actions or innocent of their actions. And prior to 1965 this was done on a charity basis by almost every doctor in the country. There were entire charity hospitals for providing care to the indigent. If it wasn’t a charity hospital almost every hospital in this country had a charity wing. Which is separate from the rest of the hospital where charity care was provided to those who needed it. But what Medicare and Medicaid wanted to do is they promised not to control medicine…”We just want to pay the bill.” But the real point of the thing was not just to take care of the elderly and the poor, the point was to spare them the humiliation of means testing. To actually spare them the humiliation of having to put their hand out and say, “I need help.” But that is the difference between a charitable act and an act of force. Putting your hand out and saying, “Can you please help me.” vs. putting a gun to someone and saying, “Give me this”.
The other thing that is did and the insurance companies rather liked this is it removed anyone over 65 from the insurance pool. So you’re a commercial insurance companies- you just took the totality of your highest risk covered lives out of your bailiwick and you don’t have to worry about it anymore. The public sector is going to take of that so your profit margins just went through the roof and it shifts the cost on the government which is you the tax-payer. Oops.
So, what are the logical consequences of that? Remember, at every step of this process when we screw up we don’t go “oops” and go back, we go, “oops” and double down. So what’s the Oops?
Baby Boomers. Holy Crap! The hugest population explosion in the history of our country was going to come to fruition under this act. So what happened is- you’re promising care to a huge number or people who paid in when it was extraordinarily cheap but you’ve created a system where the cost of providing that care has to go up exponentially. So now you have a situation where if you’re going to keep this thing propped up from one election to the next, which is very important because this is also a demographic that votes and votes with fierce self-interest very much in mind. If you doubt if the baby boom generation has screwed you young guys -they know that they were at the beginning of a Ponzi scheme. And they were more than happy to pass that debt off onto you. You’re going to pay for this with money you’re not going to earn until you are 50 years old.
So how do we keep propping this up from one election to the other? Well we have to control costs. Well we do that by limiting treatment to what is considered appropriate or medically necessary and we try to limit payment to doctors. The other thing it did is it outlawed any supplemental payment form the patient to the doctor. So they start limiting how much they pay doctors- doctors don’t want to see patients anymore. Well a lot of people that were forced into Medicare said “Eh, I’m well-to-do. I’ve got plenty of money, Doc. I’ll pay you the difference between what you get from an insurer- someone that pays out of pocket- I’ll pay you the difference between what Medicare pays you and what you would have gotten.”
Well guess what? The government will not allow the doctor to do that if he participates in Medicare. So if you take that kind of money from someone you are subject to a federal crime that is going to send you to jail and you’re going to be subject to fines which under federal law have treble damages which means that whatever they decide to fine you- you owe 3x that amount. If someone in your office finds out- there’s something called ‘qui-tam’ which is a whistle-blower statute that says not only do you pay treble damages, the person that rat-finked on you, whose payroll you meet, gets treble reward too. So you end up paying six times the fine that is levied against you. So this has huge teeth. So what’s the next thing that happened? That wasn’t enough. It didn’t stop it.
Next thing was DRGs – Diagnosis-Related Groups. This came about in 1982. And it was courtesy of a couple academics by the name of Robert Fetter and John Thompson who were public health and epidemiology experts from Yale. And they came up with this system of paying doctors in what are called diagnosis-related groups. And what they did was they standardized different diagnosis through this giant manual called the ICD which is I can’t remember what is stands for- The International Compendium of Diseases or something of that nature (International Classification of diseases ~Jimm), but what it boils down to is that if you get admitted to the hospital and you have a certain primary diagnosis you get a certain number of hospitalization – a fixed amount they are going to pay for and that’s it. And it’s on the lowest possible end of what you can be paid from something of that complexity. Well what that is, is essentially, is a price control on in-patient medical care. Remember any time you apply price controls you get shortages. This created a shortage of in-patient hospital beds because hospitals could not admit that many people into the hospital and incur those kinds of losses. They had to back off on the number of people they were admitting – make the hospital smaller, have fewer beds because they can’t take that many losses under this payment system. This is why if you go back to your home towns and you look at a local community hospital what you’ll see is this dilapidated, old ugly building that has maybe 134 beds in it. But right next door to it, you’ll see a palatial, beautiful, bigger-than-the-hospital outpatient surgery center or an outpatient radiology center or a blood collection/transfusion center. Because they’re trying to divert their activities into the out-patient setting where these price controls did not exist.
The other thing that happened is it triggered cost-shifting. If you’re going to lose that money on the in-patient side of medicine, you’re going to shift that cost to other areas. This is where you get your $200 Aspirin in the E.R. We’re trying to make up for the constraints there. You push down on a balloon on one area, it’s got to expand in another. So they’re trying to preserve market signaling in the presence of something that distorts it. So that’s going on.
Then next thing that happens is what has affected my life so immensely. 1986 – Signed into law by one of our most conservative Republican presidents in modern history – EMTALA stands for…it was part of COBRA: Congressional Omnibus Reconciliation Act of 1986. This was a sub-component of COBRA called EMTALA: Emergency Medical Treatment and Active Labor Act of 1986. And what was happening is, when you go to do a residency at a public hospital or a county hospital -residency: you’re going to specialize in internal medicine, family practice, surgery, neurosurgery, orthopedics; ophthalmology-residencies are paid for with CMS funds- with funds from the Center for Medicare Services. So that created an obligation for hospitals that had residencies because they were receiving funds and tax advantages to take care of indigent care. So in 1985, if you were a private hospital and you have an indigent person show up with a medical condition, you just tell the ambulance to do a U-turn. You go to the public hospital. They receive funds for this kind of care. Go get your care there. And that’s what happened. And that’s how the indigent paid for their medical care was by essentially being the patient for medical residents. But public funds were going to those hospitals. It was considered fair but all of a sudden the public hospitals under the effects of the DRGs were getting all these non-paying patients coming in and suffering even further loss than the constraints of the DRGs. You had non-paying people. So they started to scream and yell that this was dumping. “You’re dumping your undesirable patients on us simply because we’re good guys.” So we signed this into law and what it does now is it requires any emergency department, any E.R. to treat anyone who presents within the hospital property or 250 yards of the E.R. regardless of their ability to pay. What that also means is regardless of their intention to pay.
How quick did you think it took people to figure out how to game this system? You want to talk about viral spread of an idea? It happened overnight. The public hospitals…emptied out. They were like, “What happened? Our waiting room used to be jam-packed” and everyone was going to the more desirable hospitals because they were given a political mandate by force that they could go get that care for free. And it’s an un-funded mandate with severe penalties. There is no mechanism to pay an emergency physician for seeing this.
So what this did is it made emergency rooms the de facto national health plan for the uninsured. State and local governments abdicated all responsibility for charity care and based on statistics, that were done around 2000, they said the average Emergency physician is providing $138,000 a year in uncompensated care, I myself- when I calculate- provide approximately $350,000 in uncompensated care based on Medicare payment rates. Which as we’ve already discussed are price-controlled. So that’s the low end of the spectrum assuming that applying that, I provide about $350,0000 in uncompensated care. About 23-30%, depending on the quarter that you look at, of the patients that I see pay me anything. So this resulted in further cost-shifting just to survive. This is where you get your $200 Aspirin in the ER. And the thing is- it’s the law that was intended to help the poor hurt them the worst.
There was a massive influx of non-paying patients and that contributed to ER overcrowding. And most people when they think of an over-crowded ER, blame this scenario for the overcrowding. But I’m here to tell you it’s maybe 15% of it. Where the real overcrowding in the ER comes from is the lack of inpatient beds because of the price-controls applied by DRGs. Because the people coming into the ER are sick. There’s a lot of minor stuff that comes through and you’re always kind of turning that wheel but there is no shortage of critically ill people coming through the ER. And you have to get them. You have to stabilize them. Get them treated. Get them ready to be admitted to the hospital but guess what? There’s nowhere for them to go. There no bed upstairs. So they end up boarding in the ER. So the size of your ERs bed capacity starts to shrink. So then instead of having 20 beds to move a big back log of patients in the waiting room through, you now have ten. And in a few more hours, you’ve got five. And then you’re really hosed. So the real problem with the over-crowding is not just the massive influx of people coming in the front door, you’ve got nowhere to send them upstairs because of in-patient price controls.
The other thing that happens is the on-call doctors- the people you need for back-up- the orthopedist for the broken hip, the neurosurgeon for the gunshot wound to the head- they stop taking call. And they stop taking call because they know that when they get a call from the ER at 3 in the morning there is a 70% chance that they’re going to get up, go out of bed, take the risk of taking care this patient for no compensation, finish up that surgery and go to an office that’s backed up. So they stop taking call. So we’ve got no back up for a lot of different specialties.
Next thing that happens: 1996 – HIPAA. That stands for Health Insurance Portability and Accountability Act of 1996. And basically what this law was to do was to give Government enforcement of the Hippocratic Oath, part of which is to say: Anything that happens between the doctor and his patient remains confidential. And the reason for this is when you collectivize medicine , the ability to keep it confidential because you’re serving the collective and not the individual becomes compromised.
The other thing that was happening was the government was already planning to mandate – remember this is 1996 the internet boom was going, computers are going to solve every problem on the face of the Earth. So there is this huge governmental push for electronic medical records and they worried about sensitive personal information being stolen so they impose imposed huge penalties if you even inadvertently violated anyone’s confidentiality. I cannot practice medicine on a day by day basis without violating this law every time. If someone comes from a drug house or a rave party unconscious, whoever’s with him, you know, some kid with pink hair and a bone in his nose- I gotta drag this kid in that’s remotely their friend and say, “Here’s the circumstance with this guy -he’s dying right in front of my eyes do you know what he did?” Under this law, that’s a violation. But I have to do it every day just in order to be able to practice. It’s impossible to comply with.
But if you have something called a “compliance program”, if you hire someone to serve basically as a government rat-fink within your own organization, then if you have a slip-up, then you’ve at least demonstrated that is an honest slip up and the penalties are less severe. You have to incur essentially a full-time equivalent of hiring a person on board to make sure that you’re being HIPAA-compliant. And every time you go into your doctor’s office- the first thing they give you is this big long sheet of paper about your privacy rights that you have to sign. Anyone that’s been to the doctor’s office recently knows what I’m talking about. But this was greasing the path for the electronic medical records which I now have to deal with. This all combined, signals the death of private practice.
Overhead burden from Medicare Medicaid, private insurers, HIPAA, it eats up all of your profit margins. In the past four years, 80% of family practice doctors in my community paid themselves no salary. Of the ones that did, they paid their nurses and mid-level providers more money than they were able to net out of their practice. As a consequence, these people were bought up by hospitals who had the scale to deal with the regulatory burden. It’s wasn’t like they were brought in by a hostile take over. These people begged the hospitals to be employees because they couldn’t make it otherwise. That’s what happened. So now what you have is medicine is collectivized both on the provider and the recipient side. Control is easier. You have control of both sides of the equation from the government standpoint.
Even if this was an unintended consequence, you couldn’t have devised a more diabolical system for getting complete control.
Ultimately this created a Hospitalist movement. If you get sick in the old days, your doctor would see you in the office, say “You’re really sick, you need to be in the hospital.” He’d do a complete history, physical exam, write admission orders, send you over to the hospital, you go upstairs and he’d see you. From his office-he’d either see you immediately if it’s urgent or see you later in the evening after office hours. But your doctor who knew you intimately would take care of you in the hospital. No more. All in-patient care is shifted to hospital employees which are Hospitalist. They provide the in-patient care when the patient comes into the hospital. And this happens because the hospital practitioners that became hospital employees are now under sever scrutiny to be productive within the office and if they have to come and provide in-patient care mess up their schedule, they’re productivity falls and they get in trouble for it.
There’s also a refusal to take call because EMTALA increases their exposure to making their bottom line look bad and make them look bad and the hospital and the hospital has no conception of calculating the economic value of doing something that the government has mandated that you do. So the hospital’s been hired to provide in-patient care and these are excellent physicians. But they’re excellent physicians who’re under enormous pressure to practice for the collective rather than the individual. And to their credit what they’ve done because these are doctors – very smart people – is they have become very creative at kind of subverting the system and making it work but what happens is the Government constantly changes the rules of what they’ll pay for and what they won’t pay for so it’s always a moving goalpost. So in order to the help the Hospitalists, the hospitals now hire case managers. Case managers are usually nurses who have the good sense to get out of clinical care or social workers. And they have this big manual from the government about what they will and will and what they won’t pay for and what the diagnostic criteria for being admitted into the hospital are. And they help the Hospitalists figure out what they can and cannot do. Now make no mistake, if something doesn’t fit this template, they’re not saying you can’t admit the patient to the hospital. They can and we do all the time. They’re just saying “We’re not going to pay for it.” And when the hospital is under this much financial pressure, there’s very huge pressure to predicate your admissions to the hospital based on what’s allowed.
This was signed into law on March 23rd, 2010. I watched it while waiting in a neurologist’s office for four hours to be seen. The reason I was in the neurologist’s office is that I got a weird neuropathy. I thought it was a pinched nerve in my neck. Maybe from working out. But my intrinsic hand muscles atrophied to the point where I could no longer pinch or turn a key. One day I had a patient that went into respiratory arrest. I had to intubate them. I used a laryngoscope to expose their vocal cords and the endotracheal tube- the plastic tube we put down your windpipe- I couldn’t hold onto it as I was passing it through. And I was like, “Oh, crap-I gotta figure this out.” So I was waiting to have a nerve conduction velocity done. As it turns out I had something called Cubital Tunnel Syndrome. We were mandated to have electronic medical records or face severe financial penalties in terms of what Medicare would pay you. So, huge pressure from the hospital – we went to instead of voice-dictation that was transcribed to this computer template that you had to mouse every little bit of the patient encounter. And what is was, was a desk with a glass table top and I was raking my ulnar nerve over and over again. I never thought after 20 years of education I would have the sort of job where I would have a repetitive motion injury. But I was there being evaluated for it while as I watched this being signed into law. And the thing is that everyone’s just really up in arms about this thinking that this is going to do new and horrible things and it’s not.
Here’s what it does: is it just takes everything that horrible about our current system and mandates that you buy into it, even if you object. And the scariest thing about the latest court case is, the first time in American history someone can tax you for something you did not do. You’re not being taxed for taking an action you’re not being taxed for producing something or selling something. Or bartering any sort of transaction. You’re being taxed for an inaction.
So this includes all the negative elements of what brought us here. But the other thing it does- it shuts off any escape valve for cost shifting. Everyone’s co-opted into this thing. So what’s going to happen now is once these price controls are enacted and they cannot be dissipated by cost shifting , you’re going to have massive shortages. It’s going to be really hard to get in to see anyone or get care. So if you get sick, expect to be deflected to the ER when you go to your doctor’s office. The doctor’s office is for routine care and simple stuff. You do anything that screws up the flow of the schedule, they’re going to punch you to the ER. When you get to the ER, expect long waits because everything’s being shunted there. And EMTALA remains in effect. Call your doctor’s office. Go out in the hall; call your doctor’s office on the cell phone. (They) will say, “If you think this is an emergency call 911 go directly to the emergency department. When you get to the Emergency Department, what’s the thing the triage nurse says to you? “Didn’t you call your doctor” No one wants you. Because you are a liability to everyone involved in this system now.
If you need admission, it’s going to be a fight. We’re going to have to find a damn good reason for you to get in and we’re going to have to ram a square peg into a round hole to make sure we get some sort or reimbursement and you’ll be kicked out as soon as possible whether you’re ready or not. It’s all protocol-driven. Any time you receive a treatment it will be per protocol. If you come in chest pains, you’re going to be discharged on a statin. And if you’re not discharged on a statin, that’s going to create the physician being flagged as an outlier and a troublemaker.
The sicker you are the more you’re viewed as a liability. Be prepared to be discharged prematurely. Come in with pneumonia, you’re not completely better, but maybe good enough, they’ll send you home and right now we’re experiencing multiple ambulance u-turns. And what I mean by that is almost every single shift I work I will see at least one ambulance patient that was someone that was discharged from a hospital being driven home in an ambulance that has to do a U-turn and come back because they are decompensating. Guess what? If you’re at risk of re-admission within 48 hours, they ain’t paying. So now the re-admission is even more of a fight than the original admission because no matter what you do, no one’s getting paid. But lots of people are doing the U-turn because of the premature discharges. And understand this is not because the doctors aren’t good. These are extraordinarily smart and well-meaning people. They’re just operating under the constraints of enormous pressures.
So remember, he who holds the gold makes the rules. What becomes protocol is subject to lobbying groups. And what treatments are approved are influenced by Big Pharma. Big Agri is subsidized corn and you end up “needing” Lipitor and “needing” Glucovance. And what lands most people in the hospital is the dietary habits that are created by a Big Agri and the USDA. And you get admitted into the hospital what they bring to feed you will be what the USDA says to feed you.
So remember getting sick – it’s always meant a loss of control but now it means a loss of control and a loss of your liberty. Your doctor no longer serves you. He serves the collective. His compliance is strongly coerced if not forced. Currently it is coerced very strongly. Soon it will be forced. And remember you are a financial loss to everyone involved. It’s cheaper if you die. As long the protocol was followed it’s in your best interest to be a quick healer. That’s why you want to eat the Paleo diet. That’s why you want to do high intensity exercise. That’s why everything that we talk about here is so important. You do not want to get in the belly of this beast.
So, you doubt me? Take the airport test. When you guys are flying back home, look around. The vast majority of people are already within the belly of the beast. And that’s the thing that always cracks me up when you hear, you know, fitness guys that get up here and say, “I’m going to change the healthcare system. We’re going to be more about prevention and health than we are about disease.” Come to work with me one day.
You. Have. No. Idea. How sick people are.
I saw a 48-pound two year old with Type 2 diabetes. At Walmart you can buy nipples that screw on to a Mountain Dew Bottle. Look around you. Just walk out front look at someone out in the smoking area that’s you know, a hundred pounds over-fat. And realize- this person gets the flu? They’re going to be real sick. The onslaught of sick people that need big Pharma-type interventions because it’s all predicated and focused on that sort of recovery from the brink. There is so much of that coming at you so fast you don’t have any time to think of alternative medicine or prevention or anything like that. Doctors are buried by this. So being fit and medication free gives you an enormous competitive advantage and it subverts dependency. Direct control over your life is removed. It leaves you in a much more resourceful mode of being able to deal with the multiple indirect controls that are being exerted over you right now.
So how do you do it? Eat a Paleo diet.
And you don’t have to eat Paleo.
What that means is “avoid Neolithic agents of disease”. Eat nutrient dense whole foods. Single-ingredient diet. You should eat something that has a single ingredient: Broccoli. Meat. Eggs. I was talking to Dave earlier and we were talking about eggs, fat and the diet and how important it was and particularly how important it is in pregnancy and gestation. Dave said, “Look at an egg. Look at a yolk. Everything you need to make a chicken is right there.” That’s nutrient density. Eat a Paleo diet. Find a book: Primal Blueprint {by Mark Sisson}. Rob Wolf’s book, The Paleo Solution. The ONE diet by Simon Shawcross who spoke in London. Primal Body Primal Mind by Nora Gedgaudas and The New Evolution Diet by Art Devany. Pick any one that appeals to you and follow it. If you respond better to visual and aural presentation, see my 21 Convention Talk on Youtube 2010. I’ll lay it all out for you in technical detail so you’ll understand both the ‘why’ and the ‘how’.
Exercise. Do high intensity, low force exercise with plenty of recovery. What Skyler told you is gospel truth. You can read my book “Body by Science”.
First, do no harm. (The Bill De Simone paper “Primum non nocere: A commentary on avoidable injuries and safe resistance training techniques” ~Jimm)
Find Bill De Simone’s work and read it. Moment Arm Exercise. You don’t want to injure yourself either. It’s not enough not to be sick. You tear your rotator cuff. Guess what? You’re in the belly of the beast. So you should avoid ballistic exercise and if they use skill based movements in a fatiguing protocol. I love the spirit of Crossfit. I love the notion of: doing-hard-things-builds-character. But what I don’t love is a fatiguing protocol with skill-based movements that are going to get you injured. Same thing with P90X or Insanity workouts. Do high intensity, low force workouts. Because injury will put you into the belly of the beast very quickly. Remember, when you’re becoming super-human, the way to do that is to remember you’re only human. And biohacking -everyone referred to it as cheating. It’s not. It’s not cheating. You’re not cheating anything.
Francis Bacon said it best: “Nature, to be Commanded, Must Be Obeyed”.
You’re obeying nature when you’re following a Paleo diet, when you’re doing what Dave Asprey tells you when you’re doing what Skyler Tanner tells you, you’re being a good animal. A cheetah doesn’t have to count his calories. A lion doesn’t count his calories. They’re in perfect metabolic and physical conditioning without even thinking about it. The same is true for us. The reason it seems like such hard work is we’ve become so far removed from the evolutionary dictates that made us what we were meant to be.
The other thing you want to do is what I call Black Swan Avoidance. Or my dirty dozen plus one. So let’s talk about them.
~~Break transcript~~
Doug humorously reviews a bunch of ways he has seen people die as an emergency room doctor and suggests ways to not get yourself into those situations. I’m not going to transcribe it at this time. But a couple of key quotes/paraphrases are:
“Force is Mass Times Acceleration. Take it from an Emergency room doctor”
“If the grill won’t light, walk away”
“The ladder. This is the white man’s scourge”
“Buy your home to retire in. Don’t build it. I see guys die of a myocardial infarction from arguing with a contractor once a week. We live in a resort area so there may be selection bias.”
“If you ever get into a car at the point of a weapon, you will most certainly die but not until you have really, really suffered.”
“Be Kind. It’s the most important thing for your health and our society.”
“Speaking of kindness-We have these huge forebrains. It’s very important for communication. And it’s what’s lacking when you communicate of the then interact or over the cell phone or by text messaging. There’s a very strange version of stroke called Aboulia, when you have a stroke in the frontal lobe of your brain. I can walk up and talk to the patient and speak to them and they just stare at me with this dead-pan face. And their answer doesn’t come out until 10 -15 minutes after I ask the question. But I can give them a cell phone and call them, step outside of the room and get a complete history from them because they’re communicating in a mechanism that is not at all facial recognition in the pre-frontal lobes of the brain. Realize that when you are communicating over the internet and you are flaming someone on the internet and you’re getting into these little pissing matches that you are not engaging your frontal lobes. You are saying things that you would never say to someone’s because you know damn well you’re likely to get punched or killed. Kindness matters. Because we all must die.”
“I’ll leave you with the words of Ron Harris who wrote The End of Faith and he said this: ‘Consider it. Every person you have ever met. Every person you will ever pass in the street today is going to die. Living long enough each of us will suffer the loss of friends and family. All are going to lose everything they love in this world. Why would we want to be anything but kind in the mean time?’”
and
“Stay Out of the Belly of the Beast”.
Doug then takes some questions and tackles subjects such as:
Walmart and it being the logical consequence of the removal or market forces (i.e. You can buy donuts right next to antacids and diabetes medication)
Sexuality and sexual health
Recommendations for health insurance (already out of date)
More details on the bureaucratic Armageddon of Obamacare
Why do other countries with socialized medicine look so cool and we don’t?
“HELL HATH NO FURY like Oxygen with unpaired electrons!!”
Ignacio Ocasio, Teagle Professor of Chemistry, CWRU
Case Western Reserve University’s beloved “Doc Oc” was a character the likes of which you meet once-in-a-lifetime.
He was renowned for his ability to know the name of almost every incoming freshman as they arrived on campus. During the CWRU application or acceptance process, students were asked to provide a photograph to the University. He would get a hold of these photos, then while teaching his summer lab class, scan each one. He would crop it to a mug shot and label with the student’s name and make this his screen saver. Then he would fly to Puerto Rico to visit his mother for the rest of the summer and write the following year’s homework while learning names sitting on the beach. Then he would return to teach another year and repeat the process as he did for over 30 years. He never married, had children or even a fish tank. His life was CWRU students. Many students coming to Case are pre-med hopefuls or engineers, so most of them had to take his introductory class.
When he returned to his office for Fall semester, several students would be waiting for him to open the door, just as they do after every class. His office was full of students all day long in perpetual Chemistry tutoring and many spent just as much time at his apartment, watching football or movies or listening to him play piano. He was the consummate carrier of CWRU Team Spirit, appearing at football games, the ‘Hudson Relays’, judging “Mr. CWRU” and attending most social events. Doc Oc was considered by many to be his or her “actual” college advisor, including by yours truly. He would look you in the eye and give you the most honest opinion a person could give (often under his breath with sidelong glances).
Professor Ocasio was also a brilliant pianist. He was actually pursuing Grad school for both Chemistry and music at the same time. I don’t remember if he went to the Peabody Conservatory or turned it down-that may be part of the story, but when his father became terminally ill, he felt that he had to chose between the two, so he chose Chemistry. One day he was asked to teach a Chemistry course for nurse and never looked back.
Things were not always easy for Doc, though. He never Published and if memory served was never tenured. So every time money problems came up, CWRU would float the idea of canning Doc Oc, prompting near riots, circulating petitions and impassioned letters to the campus newsletter, which they surely expected because it happened every time they did this. He even faced some harassment concerning his Puerto Rican heritage from some miscreant students. As a non-traditional (very old) student who actually took his introduction course twice (once in ’96 then ~2003 as a refresher concerning my employment) He talked very openly with me whereas he wouldn’t even curse around undergrads. I know a lot of his opinions of some inner-workings of CWRU and his perception of the shift in the general personality of students from 1980 to 2005. He gave me many insights and comforts in a very competitive, high-stakes environment and always made me feel that it was no B.S.-despite his manic, coming-from-all-directions, over-the-top energy that made you question if you were in the same quantum state as he (that’s a Chemistry joke).
In 2005 Doc Oc passed away suddenly at the young age of 53, anguishing thousands who responded passionately.
In morbid hilarity, Doc Oc already had his funeral-including music- planned and we followed it to the ‘T’ at Harkness Chapel with his mother and sister attending.
In 2008, We cast his likeness in Bronze by the Hudson Relays Rock, facing the incoming pathway so that he could greet all that are coming to the Quad.
The “Hey, Thanks!” Series will be about the people who made me love learning life sciences and love teaching them even more. They sit on my shoulder as I try to replicate for others what they did for me.